Today I conducted my final Sunday services under full-time appointment. The first was at Gideon UMC, the second at Greenbrier UMC, both in Greenbrier, Tennessee. After 23 years of full-time pastoring in the UMC, preceded by retiring as an artillery officer from the US Army, plus two years of employment in a BTB Information Technology compay, I will enter retired status for good this coming Wednesday. Here are some photos from this morning.
Serving Communion at Gideon. We used prepackaged, individual cups with the wafer and the wine (grape juice) wrapped together in one unit. I served with tongs so no one's hands ever touched the cups but the communicant's.
My final benediction at Gideon UMC.
When Cathy and I arrived at Greenbrier UMC, this sign awaited us near the front entrance.
Beginning my final service at Greenbrier UMC.
Consecrating the Communion elements.
My successor pastor, beginning there July 1, is the Rev. Jason Wilkerson, whom I have known since I moved to Robertson County three years ago. He is a very fine Christian gentleman and minister. I invited him and his family to attend today to introduce him to the congregation. I also asked him to assist in serving Communion.
Our Communion steward, the wonderful Donna Watkins, prepared Communion with the bread (the "chiclet" style) in trays of cups and the wine in other trays. She prepared these entirely in keeping with proper C19 protocols so that neither the bread, the liquid, nor the cups were ever touched by anyone but the recipients.
Rev. Wilkerson and I were both masked while serving and we donned new sterile nitrile gloves first. We removed each cup from the tray and handed it to the communicant so that no unprotected hands ever touched anything but their own serving.
In the photo above, I am serving Rev. Wilkerson at the end, just after he served me. This was one part of our ritual of me passing the pastoral care of the congregation to him - leaving him with the place of honor in the Methodist tradition: last. Hopefully, this helped the people understand that there is an orderly, grace-filled and indeed sacramental continuity of pastoral care of the people of God.
Then we proceeded with a litany of passing of the pastoral ministry from myself to Jason. We each led the congregation is responses and prayers for one another and the church itself.
Our closing hymn was, "Lord, You Have Come to the Lakeshore," number 344 in the UM Hymnal. This hymn was requested by a church member but coincidentally (or not!) it was also the thematic hymn of the service of Annual Conference in which I was ordained. So the hymn has always been deeply meaningful to both Cathy and me.
My final benediction to the people of Greenbrier UMC, which I basically ripped off from Paul's first letter to the church in Corinth, chapter 4. But I meant every word as if I had written them myself, although I could not have done so nearly as well as Paul did.
To the church of
God that is Greenbrier UMC, to those who are sanctified in Christ Jesus, called
to be saints, together with all those who in every place call on the name of
our Lord Jesus Christ, both their Lord and ours:
I give thanks to
God for you because of the grace of God that has been given you in Christ
Jesus, for in every way you have been enriched in him, in speech and knowledge
of every kind just as the testimony of Christ has been strengthened among you.
He will also strengthen you to the end, so that you may be blameless on the day
of our Lord Jesus Christ. God is faithful; by him you were called into the
fellowship of his Son, Jesus Christ our Lord.
The church hosted a "walk-thru" reception for Cathy and me after the service. It would have been outside had weather permitted.
A wonderful lady of the church made this for me - Wake Forest was my undergrad school. I already had a Vandy bottle. I earned my M.Div. there.
That Cathy was also in ministry with me at the churches was a real fact and the people said so! This was given to her because everyone knows (I mean really knows!) that Cathy loves to cheer for Duke basketball.
This fine family of four are special to me for two reasons. One is that I baptized all four of them when they joined the church. The other is that he is also retired from the Army and is the only other person in the church who speaks the language of acronym as I do. So we could have whole conversations without anyone else understanding a word (except probably our wives)!
The church gave us this laser-etched crystal plaque as a gift. We are deeply moved by this thoughtfulness!
The people of Greenbrier UMC very kindly made this video for Cathy and me.
Cathy and I are thankful beyond description to all the people of Greenbrier and Gideon UMCs for the past three years. A finer and more wonderful group of people with whom to come to the finish line neither of us can imagine! What is next for us? Love God, love neighbor, and leave the rest up to the Lord.
May the love of God, the mercy of Jesus Christ our Lord, and the strengthening presence of the Holy Spirit be with us all, now and always. Amen.
If we continue on the present course, we will enter a depression that might make the 1930s a distant competitor. The number of jobless Americans could reach tens of millions.
Yet the costs of this national shutdown are growing by the hour, and we don’t mean federal spending. We mean a tsunami of economic destruction that will cause tens of millions to lose their jobs as commerce and production simply cease. Many large companies can withstand a few weeks without revenue but that isn’t true of millions of small and mid-sized firms. ...
The deadweight loss in production will be profound and take years to rebuild. In a normal recession the U.S. loses about 5% of national output over the course of a year or so. In this case we may lose that much, or twice as much, in a month.
Our friend Ed Hyman, the Wall Street economist, on Thursday adjusted his estimate for the second quarter to an annual rate loss in GDP of minus-20%. Treasury Secretary Steven Mnuchin’s assertion on Fox Business Thursday that the economy will power through all this is happy talk if this continues for much longer.
This is the first time ever that the US Government has deliberately shut the economy down, and the idea that it can just be turned back on like flipping a switch is delusional.
Consider: We will never be able to determine how many lives were saved from the virus. But we will easily know how many people died because of the economic crash to come - just count increased suicides and even some homicides, to say nothing of untold numbers of people thrown into permanent poverty.
The lockdowns and stay-at-home orders are saving lives now. But if they continue much longer, they will cost lives later and cause economic, literal suffering for years and years to come.
On April 12, 1937, the express train to New York roared across the New Jersey countryside. The train, a Pennsy Railroad electric locomotive the color of bull’s blood, usually passed through the station at Elizabeth at about 50 miles per hour. On this particular morning, it came to an unanticipated stop. As the express rounded the curve, my great-grandfather jumped down from the platform, where witnesses reported he had been pacing for 10 minutes, and lay down across the tracks.
When the engineer was finally able to halt the train 100 feet past the platform, Roy Humphrey had disappeared beneath its wheels. His last act: raising his head to look at the oncoming train.
Roy was one of at least 40,000 Americans who took their own lives that year and the next, the two-year span that suicide rate spiked to its highest recorded level ever: more than 150 per 1 million annually.
The point is, there is such a thing as doing too little and also such a thing as doing too much. Doing too little against Covid-19 would be perverse and nihilistic. Society ought to devote a huge amount of resources, even if they must be commandeered from the private sector, to the protection of human life. But doing too much, or acting under the pressure to act rather than under the aim of coherently fighting disease and protecting people’s livelihoods, is potentially destructive, too. People need jobs, security, meaning, connection. They need a sense of worth, a sense of social solidarity, a sense of belonging. To threaten those things as part of a performative ‘war’ against what ought to be treated as a health challenge rather than as an End Times event would be self-defeating and utterly antithetical to the broader aim of protecting our societies from this novel new threat. To decimate the stuff of human life in the name of saving human life is a questionable moral approach.
Jesus Heals a Man Born Blind
9 As he went along, he saw a man blind from birth. 2 His disciples asked him, “Rabbi, who sinned, this man or his parents, that he was born blind?”
3 “Neither this man nor his parents sinned,” said Jesus, “but this happened so that the works of God might be displayed in him. 4 As long as it is day, we must do the works of him who sent me. Night is coming, when no one can work. 5 While I am in the world, I am the light of the world.”
6 After saying this, he spit on the ground, made some mud with the saliva, and put it on the man’s eyes. 7 “Go,” he told him, “wash in the Pool of Siloam” (this word means “Sent”). So the man went and washed, and came home seeing.
8 His neighbors and those who had formerly seen him begging asked, “Isn’t this the same man who used to sit and beg?” 9 Some claimed that he was.
Others said, “No, he only looks like him.”
But he himself insisted, “I am the man.”
10 “How then were your eyes opened?” they asked.
11 He replied, “The man they call Jesus made some mud and put it on my eyes. He told me to go to Siloam and wash. So I went and washed, and then I could see.”
12 “Where is this man?” they asked him.
“I don’t know,” he said.
The Pharisees Investigate the Healing
13 They brought to the Pharisees the man who had been blind. 14 Now the day on which Jesus had made the mud and opened the man’s eyes was a Sabbath. 15 Therefore the Pharisees also asked him how he had received his sight. “He put mud on my eyes,” the man replied, “and I washed, and now I see.”
16 Some of the Pharisees said, “This man is not from God, for he does not keep the Sabbath.”
But others asked, “How can a sinner perform such signs?” So they were divided.
17 Then they turned again to the blind man, “What have you to say about him? It was your eyes he opened.”
The man replied, “He is a prophet.”
18 They still did not believe that he had been blind and had received his sight until they sent for the man’s parents. 19 “Is this your son?” they asked. “Is this the one you say was born blind? How is it that now he can see?”
20 “We know he is our son,” the parents answered, “and we know he was born blind. 21 But how he can see now, or who opened his eyes, we don’t know. Ask him. He is of age; he will speak for himself.” 22 His parents said this because they were afraid of the Jewish leaders, who already had decided that anyone who acknowledged that Jesus was the Messiah would be put out of the synagogue. 23 That was why his parents said, “He is of age; ask him.”
24 A second time they summoned the man who had been blind. “Give glory to God by telling the truth,” they said. “We know this man is a sinner.”
25 He replied, “Whether he is a sinner or not, I don’t know. One thing I do know. I was blind but now I see!”
26 Then they asked him, “What did he do to you? How did he open your eyes?”
27 He answered, “I have told you already and you did not listen. Why do you want to hear it again? Do you want to become his disciples too?”
28 Then they hurled insults at him and said, “You are this fellow’s disciple! We are disciples of Moses! 29 We know that God spoke to Moses, but as for this fellow, we don’t even know where he comes from.”
30 The man answered, “Now that is remarkable! You don’t know where he comes from, yet he opened my eyes. 31 We know that God does not listen to sinners. He listens to the godly person who does his will. 32 Nobody has ever heard of opening the eyes of a man born blind. 33 If this man were not from God, he could do nothing.”
34 To this they replied, “You were steeped in sin at birth; how dare you lecture us!” And they threw him out.
Spiritual Blindness
35 Jesus heard that they had thrown him out, and when he found him, he said, “Do you believe in the Son of Man?”
36 “Who is he, sir?” the man asked. “Tell me so that I may believe in him.”
37 Jesus said, “You have now seen him; in fact, he is the one speaking with you.”
38 Then the man said, “Lord, I believe,” and he worshiped him.
39 Jesus said, “For judgment I have come into this world, so that the blind will see and those who see will become blind.”
40 Some Pharisees who were with him heard him say this and asked, “What? Are we blind too?”
41 Jesus said, “If you were blind, you would not be guilty of sin; but now that you claim you can see, your guilt remains.
If you like the very low gasoline prices, even though we are not supposed to drive anywhere, get used to it. Oil's spot price may drop some more, yes (it plummeted today after Thursday's highest-rate increase ever in one day). But production is going to drop. Usually, that means gas prices rise. Not this time. And that is actually very bad news.
Cheap gas and nowhere to go. That's bad.
American oil frackers operate at a loss much below $60 per barrel (depending where they are located). The largest such operation, the Permian Basin, needs about $65 per barrel to make a profit. It straddles Texas and New Mexico.
The drop in oil price was triggered by Russia's refusal to cut production at the Saudis' request. So the Saudis jacked production up to drive the price down and punish the Russians. Well, good luck with that:
After oil prices collapsed in the worst drop in nearly three decades—courtesy of the renewed Saudi-Russia rivalry on the oil market – Russia’s Finance Ministry said on Monday that Moscow had enough resources to cover budget shortfalls amid oil prices at $25-30 a barrel for six to ten years.
Not coincidentally, both the Saudis and the Russians would like to see America's frackers permanently closed and the United States to return to a major importer of oil, not net exporters as we are right now.
One way or another oil prices will rise - eventually. That seems a cloud but actually it is the silver lining. The cloud is cheap oil. Active-rig counts fell this week in the US by 160, year over year, to 722. On the other hand, US oil production remains near an all-time high at 13.1 million barrels per day. Go figure.
Analysts say that the month of April could see the largest supply overhang in the history of the oil market.
“We now expect the y/y demand loss to peak in April at 10.4 million barrels per day (mb/d), and annual demand to fall by a record 3.39mb/d in 2020,” Standard Chartered wrote in a note.
In the short run, the oil market surplus could reach a peak of 13.7 mb/d in April, Standard Chartered said, with an average surplus of 12.9 mb/d for the second quarter. The inventory buildup could reach a gargantuan 2.1 billion barrels by the end of the year, “stretching the midstream of the industry to its limits,” the bank wrote. That figure represents an upward revision of 50 percent from the 1.4-billion-barrel inventory surplus the bank predicted…just a week ago.
Other analysts have even more dramatic scenarios. Eurasia Group says demand could fall by as much as 25 mb/d in the next few weeks and months. The historic glut means that the world could run out of storage space. “The combination of weakening demand and excess supply is hardly going to be accommodated by onshore storage,” Giovanni Serio, head of analysis at Vitol, told the FT. “At a certain point…we will need to fill all the boats.”
Texas regulators are considering curtailing oil production in America’s largest oil-producing state, something they haven’t done in decades, people familiar with the matter said.
Several oil executives have reached out to members of the Texas Railroad Commission, which regulates the industry, requesting relief following an oil-price crash, the people said. U.S. benchmark oil closed around $25 a barrel Thursday.
Texas, which hasn’t limited production since the 1970s, was a model for the Organization of the Petroleum Exporting Countries, which has sought to control world-wide oil prices in recent decades. OPEC and Russia were unable to reach a deal on reducing output in response to the coronavirus pandemic, which helped trigger the current collapse in prices.
It is unclear whether regulators will ultimately act to curtail production, but staffers are examining what would be required in such an event, the people said.
Oil prices have always been manipulated by producers. Even so, at the end of the day, demand has always been in control. And now the worldwide demand has dropped like an anvil and will continue to do so. The largest users of petro products - shipping and aviation - are harboring vessels and canceling flights. That will likely accelerate.
That said, oil production is going to plummet because, as stated above, we are running out of places to put it. That does not mean that gas prices will suddenly rise. The huge over-supply will see to that. But cheap gas prices are not going to offset the real pain dropping demand will cause: higher unemployment not only of oil-industry workers, but businesses whose revenues depend on customers using oil just to buy or get to their products or locations, such as hotels, tourist attractions, airline workers, dock workers, gas station owners and workers, the list is very long.
I am not an economist by a long shot, but unless we stop our "insane over-reaction," there is going to be a lot of pain to come that 99-cent gasoline will not pay for.
Update: How low can it go? "How Low Can Oil Go? One Forecast Sees $5 a Barrel." Which means that gasoline will be not much higher than free - and yet it will be also more difficult to find because gas stations will be closing at accelerated rates as oil prices plummet.
“You have heard that it was said, ‘Love your neighbor and hate your enemy.’ 44 But I tell you, love your enemies and pray for those who persecute you, 45 that you may be children of your Father in heaven. He causes his sun to rise on the evil and the good, and sends rain on the righteous and the unrighteous. 46 If you love those who love you, what reward will you get? Are not even the tax collectors doing that? 47 And if you greet only your own people, what are you doing more than others? Do not even pagans do that? 48 Be perfect, therefore, as your heavenly Father is perfect."
TEHRAN, Iran (AP) — Iran issued its most dire warning yet Tuesday about the outbreak of the new coronavirus ravaging the country, suggesting “millions” could die in the Islamic Republic if people keep traveling and ignoring health guidance.
A state television journalist who also is a medical doctor gave the warning only hours after hard-line Shiite faithful on Monday night pushed their way into the courtyards of two major shrines that had finally been closed due to the virus. Supreme Leader Ayatollah Ali Khamenei issued a religious ruling prohibiting “unnecessary” travel in the country.
Roughly 9 out of 10 of the over 18,000 confirmed cases of the virus in the Middle East come from Iran, where authorities denied for days the risk the outbreak posed. Officials have now implemented new checks for people trying to leave major cities ahead of Nowruz, the Persian New Year, on Friday, but have hesitated to quarantine the areas.
That’s even as the death toll in Iran saw another 13% increase Tuesday. Health Ministry spokesman Kianoush Jahanpour said the virus had killed 135 more people to raise the total to 988 amid over 16,000 cases.
I have registered GUMC for its own account at Free Conference Call (https://www.freeconferencecall.com/). This will enable you to hold meetings by telephone conference call. And it really is free. (I have had my own account for a few years.)
Here is how it works:
Contact Malissa or me for the login and password.
Go to the web site above and login.
You will be presented with a page that states this info (I have removed the numbers from this image):
Then send this Dial-in Number and Access Code to your members, along with what time they should dial in.
Shortly before the appointed time, call the dial-in number. Voice prompts will ask for the access code and then the Host PIN. Once you enter them, your call is live, and others may dial in, enter the access code, and you are connected. Once everyone is on the call, hold the meeting. Hopefully we won't need to do this a lot longer, but I have used Free Conference Call for more than a few meetings over time (usually for weather reasons) and it works.
A zombie is actually dead, it is just too stupid to know it. And all it wants to do is find you, a non-zombie, and bite big chunks of flesh from your body. This turns you into a zombie, too.
Key point: Zombies are very bad! Avoid zombies, even if it means staying holed up in your house, never leaving, stocked with 500 rolls of toilet paper and all the hand sanitizer you can buy!
However, this is a Covid-19 sufferer:
Please note the difference. Covid-19 patients do not attack you. They do not eat your living tissue. They are not dead, like zombies are. The great majority of them recover and the ones who do not are too sick before death to track you down and infect you, even if they wanted to. Which they do not.
Key point: It's time to stop treating social distancing like prepping for a zombie apocalypse.
Even as Covid worsens in America - and it will - it will not cause the collapse of our civilization. Workers will still work, although many businesses and industries will take a hit. Farmers will still farm. Ninety percent of the toilet paper we use is made right here in the USA. Almost all the other 10 percent comes from Canada and Mexico.
Social distancing does not mean you can never leave your house. It does not mean that you will become infected by walking down the street. Even if you are at high-risk for the infection, it does not mean you must now stockpile 500 rolls of toilet paper and all the hand sanitizer you can get.
We are not going to run out of hand sanitizer or toilet paper. Or food. And even if you do not want to risk going to a (potentially) crowded store to buy more, someone else will go for you. Ask a family member, neighbor, friend. Ask a local church or synagogue for help.
There was never a reason for this to have occurred across the country:
In a week or so, those who did this are going to wonder why. And people who bought cases and cases of vegetables, two-dozen pounds of chicken or beef will wind up throwing a lot away, spoiled.
Buying as if there is going to be a shortage is a self-fulfilling prophecy. It is what creates the shortage.
So chill, Americans. Just chill. Take all the proper precautions against the virus. But nothing about this disease requires stockpiling. Face the future with confidence and planning, not panic. We simply are not at this point, not by a long shot:
Don't let us get there for no reason other than we act like it.
And a reminder, if I may: While our church can practice social distancing, we cannot practice financial distancing! The missions, ministries, and financial obligations of the church continue!
Please mail your regular tithe or offering to the church!
Greenbrier UMC only - online and smartphone giving can also be done.
This is an anxious time. At the request of medical professionals of Tennessee, many churches in the greater Nashville area are not gathering in person for worship for at least the next two Sundays. We very much regret doing this, but we agree with what our bishop published, "Social distancing may seem to be an unnecessary reaction to those of you who are not sick, but medical professionals are telling us that if we wait until the need is obvious – it will be too late."
Worship for Greenbrier and Gideon UMCs will be online only on March 15 and 22. So please return to this site at the regular worship hour and we will gather together - virtually!
Come learn about the "Rule of 4 Ps" for handling anxiety, worry, and concern. Anxiety is inevitable. It is how we respond to anxiety that makes it so. How we respond makes all the difference. Here is what Saint Paul had to say about anxiety in Philippians 4:
Rejoice in the Lord always. I will say it again: Rejoice! 5 Let your gentleness be evident to all. The Lord is near. 6 Do not be anxious about anything, but in every situation, by prayer and petition, with thanksgiving, present your requests to God. 7 And the peace of God, which transcends all understanding, will guard your hearts and your minds in Christ Jesus. -- Philippians 4.4-7
Come back here tomorrow for a new and complete worship experience!
There is an old Army saying we would joke with one another in times of stress or danger, “When everyone around you is losing their heads, and you’ve kept yours – well, then, you simply do not understand the situation!”
Perhaps the most stressful word in our language today is “Coronavirus,” also called Covid-19 (Coronavirus disease 2019). It seems to have come out of China so suddenly, and so apparently lethally, that we can almost understand how the ancient Egyptians might have felt coping with the plagues because they would not let the children of Israel go.
Fear or faith? Or fear with faith?
There are many admonishments and teachings about fear in the Bible. Some examples:
•Isaiah 41:10 – Fear not, for I am with you; be not dismayed, for I am your God; I will strengthen you, I will help you, I will uphold you with my righteous right hand.
•2 Timothy 1:7 – For God gave us a spirit not of fear but of power and love and self-control.
•Psalm 34:4 – I sought the Lord, and he answered me and delivered me from all my fears.
So, is fear a reasonable response by Christian people to the onset of this virus? Is fear of this virus something Christian people may experience while remaining faithful to God?
I say the answer to both questions is yes.
Fear is an emotional response to uncertainty or threat. And the virus is a threat, though to what degree is still uncertain. The cautions against fear in Scripture do not tell us never to experience such reactions. They do tell us not to be governed by fear but to be self-controlled and reliant on God to sustain us mentally and emotionally. “Perfect love,” says 1 John 4.18, “drives out fear.” That does not mean that because we love God and one another, we are magically immunized from the virus. It means that through love we will govern what we do far better than through fear. After all, “God has not given us a spirit of fear, but of power and of love and of a sound mind” (2 Timothy 1.7).
But let me be clear about this, too: this virus has the real potential to be very serious in the United States. I will not repeat the estimates of possible infections that we have heard. They vary wildly and I have no credentials either to rebut or affirm them.
Instead, I want to say what I will do as your pastor regarding our life together, particularly when we gather for weekly worship.
We Gather Together - wait, can we still do that?
First, whether there is coronavirus or not, persons who are ill for any reason should stay home and tend to themselves. In the present day, though, being ill from any cause heightens vulnerability to the virus.
The virus attacks the elderly more harshly than the young and is more serious for anyone already dealing with other conditions, such as heart issues, diabetes, and medical (not physical) disorders. So, if such persons elect to suspend attending worship for awhile, I cannot argue with them.
That said, I hope everyone will understand that there is no special threat from going to church that is not found anywhere else. So, suspending church attendance for a time will do no good if one keeps a full schedule of activities the rest of the week!
At the church
Starting this Sunday, I will not shake hands with anyone at church (or, well, anywhere else). I will instead greet you with the centuries-old hand sign of Christian benediction, with the thumb and two fingers representing the Father, Son, and Holy Spirit.
Second, I will try to minimize us handling hymnals and other objects in the sanctuary as much as we have done until now. This will likely cause abbreviated congregational singing for a time. We may simply sing hymns by request – at least the first verse or so! But weekly cleansing of hymnals is not practical.
This Saturday, I will personally go to both sanctuaries and sanitize pew backs, doorknobs, and other surfaces that are “common touch” by worshipers. I will not refuse volunteers to help for the long term!
We will stop passing the offering plates and instead place them at both ends of the sanctuary so you may leave your offering there when you enter or exit.
We will use online media such as YouTube and our Facebook page to worship "virtually," though simulcasting is probably not in the cards.
What about Communion?
We will continue to serve Communion exclusively with individual pieces of bread and separate cups, as is our usual practice. But no one will make physical contact with either the bread or the wine except you, when you consume them. Servers will use small tongs to place a Communion wafer in your hands and we will take similar precautions with the cups.
What can we all do now?
Pray.
Serve one another in love. Persons who are in the elevated risk by age or condition – please call me if you do not want to take the risk of going to the store for groceries or other essentials and I will go for you.
Take precautions to protect yourself.
Rely on God for strength not to be governed by fear.
Worship in Spirit and in truth.
Sorry, but this needs to be said, also
As I said, I will take no issue with persons not attending worship because of concerns over the virus. But there is no delicate way to put this: even if you stay home, your tithe or offering should not.
The missions, ministries, and financial obligations of the church are ongoing. You may mail your offerings to the church or use our online giving service at https://get.tithe.ly/, or just scan this QR Code on your smart phone:
I close with a note from my colleague and friend, the Rev. Jeremy Squires:
Jesus’ message is unique because of its excessive amount of concern for the vulnerable. At its best, the Church has championed the cause of the “least of these”, as Matthew 25 has it. Christians are rarely more incarnational than when they say: society may consider you expendable, but we won’t.
No matter what the future brings, God is already there. There is nothing that can separate us from the love of God in Jesus Christ!
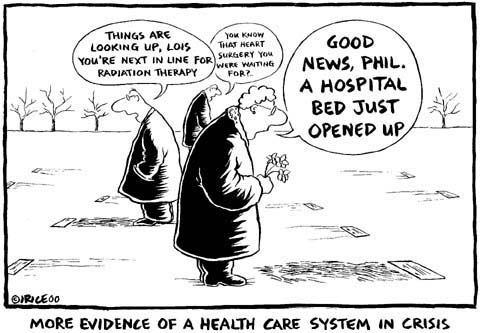
I first wrote this in 2009, but it seems relevant to today as well; I have updated it. Is health care a human right, as the United Methodist Church says? I don't see how. Human rights, as Americans have always understood them (beginning with Thomas Jefferson and the other Founders) are a fact of nature that cannot be rescinded by human beings. Rights are immutable, indeed, unalienable ("Not to be separated, given away, or taken away" Dictionary.com, as Jefferson wrote in the Declaration of Independence.) As a precursor to his Declaration theology that unalienable human rights are a endowment by God, Jefferson wrote in his pre-revolution essay, Summary View of the Rights of British America, " The God who gave us life gave us liberty at the same time. The hand of force may disjoin, but cannot destroy them."
Since his day, and certainly preceding it, the historic American understanding of human rights is the exercise of individual freedom, especially in the political realm, for both public and personal good. We have historically never understood our rights as encompassing access to services or commodities.
Rights are inherent in each individual equally, they are not divisible. Take the Declaration's famous insistence that among human rights is "the pursuit of happiness." Note that it is the pursuit of happiness that is a right, not the achievement of it. Nor is one person more entitled to pursue happiness than another, no matter one’s station in life. Besides, happiness (what Jefferson meant was not happiness as we use the word today, but a state of contentment in life and possessions) is not something that can be given us, it is something we have to create.
It does sound all high-minded to say that, like rights, health care should be equal for everybody, which I suppose is why clergy are so susceptible to say so. It's more than obvious that no one in the Congress or the White House believed it in 2009 when Obamacare was enacted. If they had, the act would have required members of Congress and the rest of the federal government to fall under the "public option" along with the rest of us proles. But they’ve protected their turf completely and much better turf is theirs than ours. I’ll believe that equal access and care for everyone is a moral imperative when the people who say it is a moral imperative place themselves under the same imperative.
The presumption that health care is a right, and therefore must be equal for everyone, is founded on two critical errors of understanding. The first is that health care is a resource that is simply available for those who need it, or that can be made equally available through proper legislation and regulation. The second error is that medical care and access to it can be rationed by command more equally, economically and fairly than by demand.
Health care is not a resource to be exploited
Medical facilities and doctors are not phenomena of nature, like water or petroleum are. Hospitals don’t just appear. They are produced. Medical care is not a resource that can be "mined" through more regulation to be more plentiful. Medical care is a service.
Specifically, it is a contracted service, in much the same way that legal assistance, automotive maintenance or pastoral care are services. Why? Because men and women choose of their own accord to get medical training. Once graduated, doctors, nurses, paramedics and technicians of various kinds reasonably expect that they will be compensated at a rate greater than their costs to enter the profession, greater than their extremely high overhead to run the practice, and enough to make their grueling hours materially worthwhile for themselves and their families.
This fact has very direct consequences under the Medicare and Medicaid systems we have today. The Atlantic's business journalist Meg McArdle explains:
[W]e have a comprehensive national health care plan for seniors. Yet we have a shortage of geriatricians, the one specialty that you would think would be booming. Why? Because Medicare sets a single price for the services of geriatricians, and it is low. Since the field is not particularly enticing (though arguably it really should be, since geriatricians have extremely high job satisfaction compared to many more popular specialties), very few people go into it. It's one of relatively few specialties that consistently has most of its slots and fellowships unfilled.
Moreover, the skills and equipment a doctor or hospital possess are their individual property, not the property, even partially, of the state or public. (There are publicly-owned facilities such as VA hospitals, but in operation there is no difference to the general public between them and private facilities). No one has a natural right to someone else's property. To think we do directly violates the Tenth Commandment. As McArdle says, "People have no obligation to perform labor for others. I may not [justly or legally] force a surgeon to save my mother at gunpoint."
That means that to receive a doctor's services, the doctor and a patient must come to a mutually-agreeable arrangement of what medical care will be provided in exchange for a specified fee. This is a commercial transaction no different in type than hiring a plumber, cab driver or lawyer. That medical services may be life critical does not change the fundamental nature of the contract.
We have access to medical care only as long as a doctor is willing to provide it. No one has to become a doctor or continue in medical practice. If any "reform" of the present health care system reduces the rewards of practicing medicine or complicates the practice, fewer men and women will so choose. Access will then go down for everyone and costs will inevitably rise, no matter what the rate-payment of the public option is, because access or its lack is itself a cost and also drives other costs.
Health care is a service
As Michael Keehn explains, health care is a service but not a community service. Police and fire departments provide community services. That seems obvious enough, but consider: fire departments do not protect your home individually. The fire chief definitely will let it burn to the ground if firefighting needs are greater elsewhere in the town. Just look at what is happening near Los Angeles as of the date of this post. Police and fire protection are in fact rationed to protect the lives and property of the greatest number of people possible with the resources available. But when the resources (manpower, equipment or money) run out, individuals are exposed to greater danger or loss though the community at large may still be protected.
Individual residents of a city do not contract for their community’s police or fire protection. When you call 9-1-1 because someone broke into your home while you were in bed, you don’t have to sign a contract with the police when they arrive, specifying the actions you want them to take and how much you are going to pay.
In contrast, medical care is an individual service. Doctors do not provide their services to the community as a whole, but to individuals. Because of that, each patient enters into a contract with his/her doctor specifying the medical services to be received and how much it will cost. This is mostly mediated through insurance companies, of course, which greatly simplifies the contracting process. The result is that a patient 's health is protected in a way that their safety or homes are not protected by the police or fire departments.
Interestingly, the Roman Catholic Church rejects the idea that health care is a human right. The Most Reverend R. Walker Nickless, bishop of the Diocese of Sioux City, Iowa, explains.
[T]he Catholic Church does not teach that “health care” as such, without distinction, is a natural right.
The “natural right” of health care is the divine bounty of food, water, and air without which all of us quickly die. This bounty comes from God directly. None of us own it, and none of us can morally withhold it from others. The remainder of health care is a political, not a natural, right, because it comes from our human efforts, creativity, and compassion.
Like any human endeavor, health care is finite. It can be properly understood only as such. Any reform that treats medical care as if it can be made infinitely available is a product of cloud-cuckoo land. Medical care, like every other finite thing, must be allocated. The current buzzword for that is "rationed." That’s the foundation of the second critical mistake people are making about health care, that medical care and access to it can be rationed by the government more equally, economically and fairly than by consumers. Philip Barlow, Consultant neurosurgeon at Southern General Hospital, Glasgow, explains why "Health care is not a human right."
Update, March 2020: In 2009. Philip Niles wrote that the real question is not whether health care is a human right, but "How much health care is a human right?" His essay is no no longer online. It is a good question because since medical care is finite. He says,
With all of the emotional and financial investment in health care, it is important to address the situation with an actionable approach - not an ideologic one. My suggestion is to quantify just HOW MUCH health care we believe is "right" to provide, recognize that we should cap public health care spending, and focus the moral/fiscal debate on how high that cap should be set. Let's achieve our ambitions of providing access for the uninsured with the most likely way of succeeding: by haggling about the price.
There is always a price to be paid, one way or another. What politicians seeking votes seem to do is ignore that price (paid by the consumer) and cost (borne by the provider) are not the same. When a political candidate promises free health care for everyone, they conveniently ignore that free care is simply, literally impossible. Look at it this way: as I write, we are in the midst of the coronavirus concerns, with a few thousand died from it worldwide and several in the US, where cases are rising. Now imagine you are a government-employee administrator for Medicare For All the next time such a potential pandemic arises -- and most assuredly there will be a next time. You have to choose between funding two heart-replacement surgeries plus rehab routines or funding the testing of 50,000 potential virus infectees for the illness. You do not have the funds to do both.
Which do you choose? Why? And what do you respond when the untreated persons demand it anyway because it is a human right? There is always this question: Who pays and in what coin? One candidate this year had either the temerity (or carelessness) to tell his audience the day before the S.C. primary, "Your taxes are going to be raised" to pay for Medicare For All. How much will taxes be raised? He did not say, but presumably they will raised an amount corresponding to the cost of providing the medical care to the population. In other words, everyone will still pay an insurance premium now called taxes, and the tax rate will never go anywhere but up. Why? Because every other nation with "free" health care finds it over-utilized and under-resourced. Take Canada, for example, which many politicos say can be a model for us. In reality ...
... Canadians' out-of-pocket health costs are nearly identical to what Americans pay—a difference of roughly $15 per month. In return, Canadians pay up to 50% more in taxes than Americans, with government health costs alone accounting for $9,000 in additional taxes per year. This comes to roughly $50 in additional taxes per dollar saved in out-of-pocket costs. Keep in mind these are only the beginning of the financial hit from "Medicare for All."
Canada's public system does not cover many large health costs, from pharmaceuticals to nursing homes to dental and vision.As a result, public health spending in Canada accounts for only 70% of total health spending. In contrast, Medicare for All proposals promise 100% coverage. This suggests the financial burdens on Americans, and distortions to care, would be far greater than what Canadians already suffer. ...
More serious than the financial burdens is what happens to quality of care in a government-run system. Canada's total health costs are about one-third cheaper than the U.S. as a percent of GDP, but this is achieved by undesirable cost-control practices. For example, care is ruthlessly rationed, with waiting lists running into months or years.The system also cuts corners by using older and cheaper drugs and skimping on modern equipment. Canada today has fewer MRI units per capita than Turkey or Latvia.
Moreover, underinvestment in facilities and staff has reached the point where Canadians are being treated in hospital hallways.Predictably, Canada's emergency rooms are packed. In the province of Quebec, wait-times average over four hours, leading many patients to just give up, go home and hope for the best.
The piper must always be paid. And so it shall be for us, but both in currency and in other than money. Medical care is always rationed. Always. And the rationing takes place within three areas:
Price to the consumer, presently mediated through
insurance premiums and co-pays, and
Medicare and co-pays and Medicaid.
Under MFA, those will be taxes and HHS.
Quality of the care provided, mediated through
the training of the physicians, nurses, and other medical staff
the quality and availability of medical supplies and equipment.
costs of the providers as related to price to the consumers.
Availability of the care, mediated
always through the number of practitioners and where they work, and that is almost always mediated through compensation,
and by what medical specialties they practice, noting that this is heavily related to compensation also (see Megan McArdles' observation above).
by limiting or even eliminating medical for some demographics, say by age, as now-suspended presidential candidate Mike Bloomberg said explicitly.
What we are falling into in this debate is the "Do something!" fallacy:
The status quo is deficient, so something must be done!
This is something.
Therefore, this must be done.
Absolutely anything can be justified by that template - and is being justified. But remember: medical care is always rationed, either by price and cost, or by quality, or by availability. When we go to the polls in November, we will not be voting for free health care for everyone. We will be voting only for how we want health care rationed in the coming years, and we will be merely hoping without any evidence anywhere in the world that it will be better than what we have now.
Health care is a scarce resource, and all scarce resources are rationed in one way or another. In the United States, most health care is privately financed, and so most rationing is by price: you get what you, or your employer, can afford to insure you for. But our current system of employer-financed health insurance exists only because the federal government encouraged it by making the premiums tax deductible. That is, in effect, a more than $200 billion government subsidy for health care. In the public sector, primarily Medicare, Medicaid and hospital emergency rooms, health care is rationed by long waits, high patient copayment requirements, low payments to doctors that discourage some from serving public patients and limits on payments to hospitals. The case for explicit health care rationing in the United States starts with the difficulty of thinking of any other way in which we can continue to provide adequate health care to people on Medicaid and Medicare, let alone extend coverage to those who do not now have it.
Consider how long it takes to get care at the emergency room in Britain. Government data show that hospitals in England only saw 84.2% of patients within four hours in February. That's well below the country's goal of treating 95% of patients within four hours -- a target the NHS hasn't hit since 2015.Now, instead of cutting wait times, the NHS is looking to scrap the goal. ...
The NHS also routinely denies patients access to treatment. More than half of NHS Clinical Commissioning Groups, which plan and commission health services within their local regions, are rationing cataract surgery. They call it a procedure of "limited clinical value."It's hard to see how a surgery that can prevent blindness is of limited clinical value. Delaying surgery can cause patients' vision to worsen -- and thus put them at risk of falls or being unable to conduct basic daily activities.
"It's shocking that access to this life-changing surgery is being unnecessarily restricted," said Helen Lee, a health policy manager at the Royal National Institute of Blind People.
Many Clinical Commissioning Groups are also rationing hip and knee replacements, glucose monitors for diabetes patients, and hernia surgery by placing the same "limited clinical value" label on them.Patients face long wait times and rationing of care in part because the NHS can't attract nearly enough medical professionals to meet demand. At the end of 2018, more than 39,000 nursing spots were unfilled. That's a vacancy rate of more than 10%. Among medical staff, nearly 9,000 posts were unoccupied.
But don't worry. We will be promised that it will different here. But there is zero reason to believe that American politicians and bureaucrats are magically more generous, more compassionate or smarter than Britain's. Or for that matter, Canada's, where the government determines medical care, and so uses that power to favor selected constituencies. In Canada, rare but expensive medical treatments go grossly underfunded while the government spends enormous sums on cheap treatments and meds that vast numbers of voters use. Like this:
A girl who died of leukemia was given a final send off after her friends signed her casket with loving messages on January 30.
[…]Laura might have experienced a few more milestones if a Hamilton, Ontario, Canada, hospital had been able to accommodate a bone marrow transplant for the young woman.Numerous donors were a match with Laura and ready to donate, but Hamilton’s Juravinski Hospital didn’t have enough beds in high-air-pressure rooms for the procedure.Hospital staff told her they had about 30 patients with potential donors, but the means to only do about five transplants a month.
[…]Dr. Ralph Meyer, Juravinski’s vice-president of oncology and palliative care, told Ontario’s TheStar.com there are plenty of others facing the same situation as Laura in Canada.
Free birth control immediately? Check. Free needles to inject illegal narcotics? Check. Free condoms? Check. Free abortions on demand? Check. Life-saving operation for a single leukemia patient? Not a chance. Leukemia patients are too few to form a voting block, so let 'em die. Then there is the Catholic-run hospice in Canada that the government is requiring closure because it refuses to kill its patients.
A hospice in Canada has lost its funding and is being forced to close after refusing to offer and perform medically assisted suicides.The Irene Thomas Hospice in Delta, British Columbia, will lose $1.5 million in funding and will no longer be permitted to operate as a hospice as of February 25, 2021.
Fraser Health Authority, one of the six public health care authorities in the province, announced on Tuesday that it would be ending its relationship with the hospice over its refusal to provide medically assisted deaths to its patients.
Anyone who thinks that none of this can happen under Medicare For All is living on a different planet than the rest of us.

































{kind=link}